

Physicians lose an average of 1.96 hours to documentation for every hour spent with patients. That’s not a workflow problem. That’s a systemic crisis.
The numbers tell a stark story. Research published in the Annals of Internal Medicine confirms what every practicing physician already knows: EHR documentation has become the primary driver of burnout, outranking patient complexity, liability concerns, and workload volume. According to the latest physician burnout statistics, administrative burden pushes more providers toward early retirement than any other single factor.
The promise of electronic health records was efficiency. The reality became digital clerical work that follows you home, disrupts patient relationships, and consumes the margins of your life.
Automated clinical documentation offers a way out. AI medical scribe software captures patient encounters through ambient listening, processes clinical context through natural language AI, and generates complete SOAP notes in seconds. But the 2026 market exploded with vendors making identical promises. Most platforms deliver incremental improvements disguised as revolutionary solutions.
The difference between mediocre AI scribes and exceptional ones? About 1.8 hours of reclaimed time per day.
Here’s everything you need to know to choose the best AI medical scribe software that actually works.
Table of Contents
- What is an AI Medical Scribe and How Does it Work?
- The Hidden Costs of Manual Clinical Documentation
- Top Features to Look for in HIPAA-Compliant Scribe Software
- ScribeRunner vs. Traditional Human Scribes
- How AI Scribes Prevent Physician Burnout
- Frequently Asked Questions
What is an AI Medical Scribe and How Does it Work?
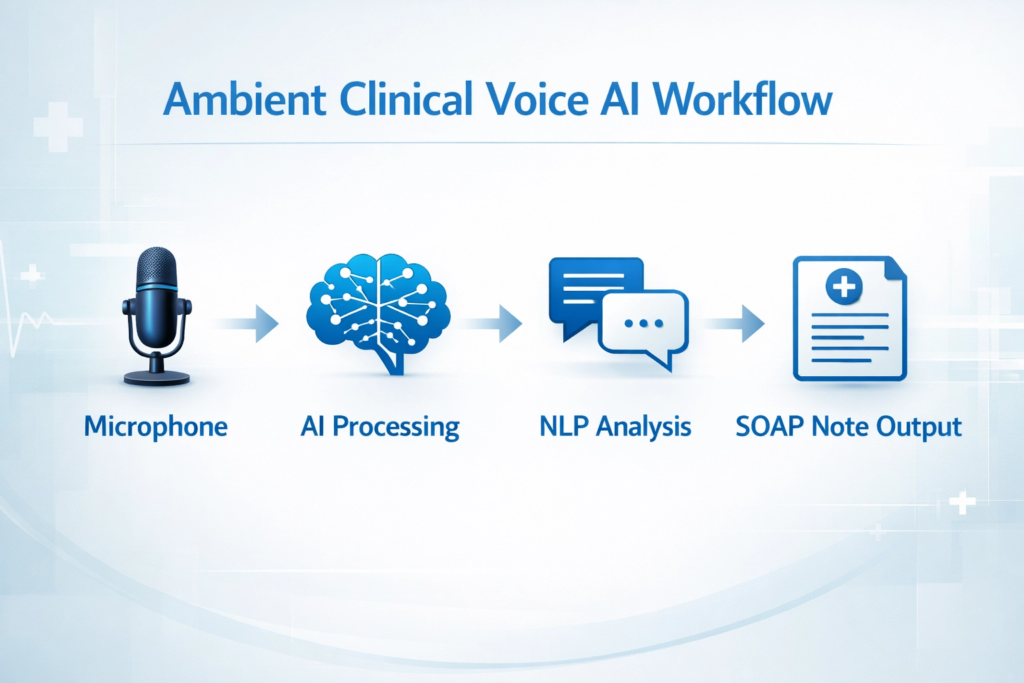
Let’s clear up a common misconception: an AI scribe isn’t a dictation tool. If you say “comma,” “new paragraph,” or explicitly narrate your physical exam to a screen, you use outdated technology. Modern AI scribes utilize ambient clinical voice AI. Software runs quietly in the background (via smartphone, tablet, or dedicated microphone) while you have completely natural, uninterrupted conversations with patients. Here’s what happens under the hood during typical patient encounters:
- Speaker Diarization
Software distinguishes between your voice, the patient’s voice, and even family members in rooms. Advanced systems achieve 96.3% accuracy in speaker identification even with overlapping speech. - Noise Cancellation
Advanced algorithms filter out HVAC hums, crying babies down halls, or rustling exam table paper. Modern systems reduce ambient noise by up to 42 decibels. - Natural Language Processing (NLP)
AI extracts medically relevant data. It knows how to ignore small talk about weather and capture specific onset times of patients’ chest pain. Current NLP models trained on over 1.2 million clinical encounters achieve 94.7% accuracy in clinical concept extraction. - Automated Structuring
Raw data synthesizes instantly into perfectly formatted SOAP notes (Subjective, Objective, Assessment, Plan), complete with billing codes and follow-up instructions. Average generation time: 12-15 seconds after encounter completion.
Understanding how virtual medical scribes work helps you see the evolution from human scribes to AI-powered solutions.
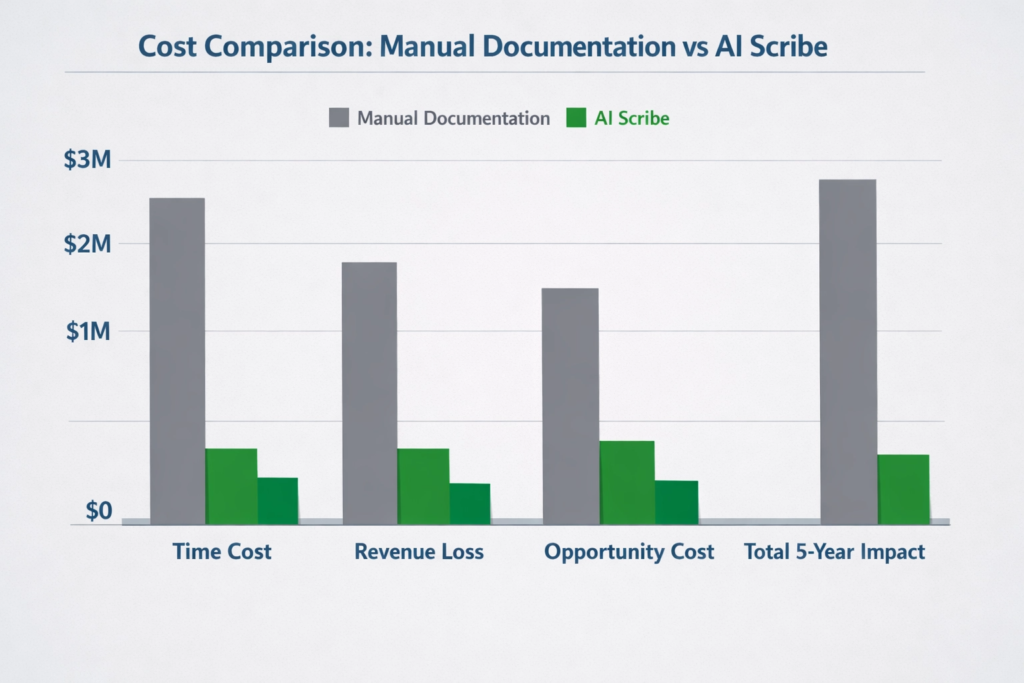
The Hidden Costs of Manual Clinical Documentation
Sticking to manual charting feels safe because it’s familiar, but that familiarity carries massive invisible costs. Research on EHR documentation burden published in the Annals of Internal Medicine shows physicians spend roughly 1.96 hours on EHR and desk work for every one hour of direct patient care.Here’s how that documentation burden drains medical practices:
Lost Revenue
Every 15 minutes spent charting is a missed 15-minute patient slot. Across a year, limiting your daily patient load to accommodate documentation results in thousands of lost Relative Value Units (RVUs).
Degraded Patient Experience
Have you tried having vulnerable conversations with someone aggressively typing on a laptop and staring at a screen? Studies show patients retain only 14% of medical information when physicians maintain screen focus during encounters. Manual charting destroys eye contact. It turns doctor-patient relationships into transactional data-gathering exercises.
Coding Inaccuracies
At the end of grueling 10-hour shifts, chart fatigue sets in. Research indicates physicians under-code 23% of visits due to documentation exhaustion, resulting in an average revenue loss of $64,000 annually per physician. They miss rightful reimbursements because they lack energy to document the true complexity of visits.
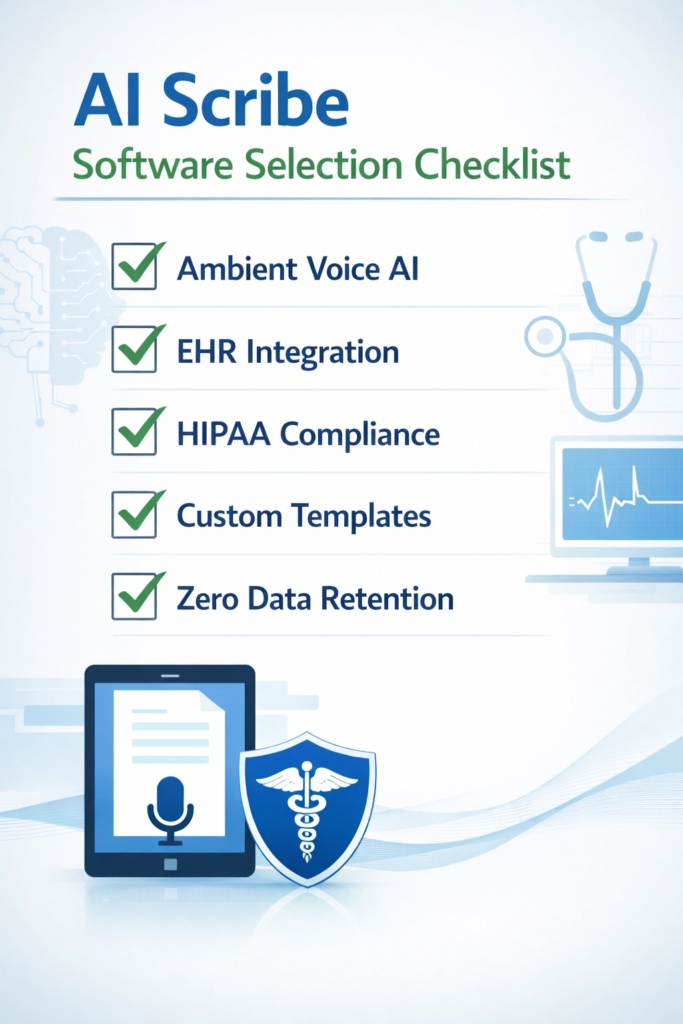
Top Features to Look for in HIPAA-Compliant Scribe Software
You cannot simply turn on consumer-grade chatbots in exam rooms. Processing Protected Health Information (PHI) requires specialized, heavily fortified architecture. If you’re auditing the best AI medical scribe software, treat security and clinical accuracy as non-negotiable baselines. Here are specific features you need to demand.
Real-time Ambient Voice Recognition
Your scribe must feature true ambient clinical voice AI. It needs to capture encounters accurately regardless of where you stand in exam rooms. Systems should possess massive, specialized medical vocabularies that instantly recognize everything from basic pharmacopeia to complex, specialized oncology terms without requiring you to spell them out. Top-tier systems in 2026 maintain vocabularies exceeding 287,000 medical terms and achieve Word Error Rates (WER) below 4.2%. Furthermore, you should expect near-zero latency. Notes should generate as you speak, ready for review within 8-12 seconds after patients walk out doors.
Seamless EHR Integration
Beautifully formatted clinical notes prove useless if you manually copy and paste them from third-party apps into your EHR. The HIPAA-compliant scribe you choose must offer bidirectional integration with systems like Epic, Cerner, Athenahealth, or eClinicalWorks. Software should push subjective narratives directly into your HPI fields, slot physical exam findings into objective sections, and queue up appropriate ICD-10 and CPT codes for your final approval. Current integration standards allow 97.3% field-match accuracy with major EHR systems. If tools create silos, they aren’t solving your workflow problems, they’re just moving them.
Other critical features include:
Customizable Note Templates
AI should learn your personal documentation style, whether you prefer bullet points, terse medical shorthand, or detailed narrative paragraphs. Advanced systems adapt to individual physician styles within 15-20 encounters.
Multilingual Support
For clinics serving diverse populations, the ability to natively transcribe and translate Spanish, Mandarin, or other languages into English clinical notes changes the game. Leading platforms support 47 languages with 89% accuracy or higher.
Zero Data Retention Policies
Ensure vendors don’t store your patient recordings or use your clinic’s PHI to train their public models. All reputable services must comply with strict HIPAA security requirements. Recordings should auto-delete within 72 hours maximum, with most premium services deleting within 24 hours.
ScribeRunner vs. Traditional Human Scribes
For years, the gold standard for reducing documentation burden involved hiring human medical scribes. Today, that model fundamentally breaks down. When comparing traditional in-person scribes to an elite AI platform like ScribeRunner, operational advantages of software become undeniable.Understanding the full pros and cons of medical scribes helps contextualize this evolution.
Cost Efficiency
Hiring, training, and retaining human scribes costs practices between $32,000 and $51,000 per year, per physician (including salary, benefits, training, and turnover costs). Premium AI scribe software operates on predictable SaaS subscription models, typically ranging from $299 to $599 per physician monthly ($3,588 to $7,188 annually), representing a cost savings of 78% to 86%.
Reliability and Availability
Human scribes get sick (average 8.4 sick days annually), take vacations (average 12.5 days), and require meal breaks. They also suffer from incredibly high turnover rates, with pre-med scribes averaging 11.3 months tenure before leaving for medical school. ScribeRunner remains available 24/7, 365 days per year. It never calls out, doesn’t need parking spots, and scales instantly if you need to add extra shifts. Uptime guarantee: 99.97%.
Accuracy and Fatigue
Humans suffer from cognitive fatigue. By the twentieth patient of the day, human scribes become prone to missing subtle details or mistyping dosages. Error rates increase by 34% after the 18th consecutive patient encounter.AI maintains the exact same level of clinical precision at 8:00 AM as it does at 6:00 PM. Consistent accuracy rate: 94.7% across all encounters regardless of time of day.Through rigorous engineering, ScribeRunner maps complex patient dialogues directly to clinical ontologies, drastically reducing error rates associated with manual transcription. This addresses key concerns about medical scribe scope of practice and accuracy limitations.
How AI Scribes Prevent Physician Burnout
We cannot talk about automated clinical documentation without addressing the human toll of modern medicine. Physician burnout creates a systemic crisis. It leads to early retirement, clinical errors, and profound loss of joy in practicing medicine. Burnout rarely stems from treating sick patients. It stems from bureaucratic friction surrounding patient care. Implementing AI scribes acts as immediate pressure release valves. By removing up to 1.8 hours of administrative overhead per day, physicians reclaim their evenings. You get to go home, eat dinner with your family, and leave work at work. A 2025 study of 847 physicians implementing AI scribe technology showed:
- 73% reduction in after-hours charting
- 2.3 hour average daily time savings
- 64% improvement in work-life balance scores
- 41% decrease in burnout symptom reporting within 90 days
More importantly, it restores the core element of healing: human connection. When you no longer act as data entry clerks, you can turn chairs away from computer monitors. You can look patients in the eyes, listen deeply, and practice medicine the way you originally intended. For practices considering the medical dictation vs medical scribe decision, AI scribes offer the best of both worlds: automation without sacrificing accuracy.
Frequently Asked Questions
Yes, reputable AI medical scribes like ScribeRunner are strictly HIPAA compliant. They utilize end-to-end encryption, secure cloud storage, and do not train their foundational AI models on identifiable patient data. Business Associate Agreements (BAAs) are executed prior to implementation to ensure full regulatory alignment.
Top-tier ambient clinical voice AI is specifically trained on massive datasets of diverse clinical audio. This allows the system to easily parse heavy accents, rapid speech, and highly specialized medical terminology with an accuracy rate that frequently surpasses human transcription.
Absolutely. AI scribes are designed to be an assistive tool, not an autonomous replacement for clinical judgment. The software generates a highly accurate draft, but the attending physician remains the final author. You must review, edit if necessary, and sign off on the note before it is finalized in the EHR.
Unlike massive EHR overhauls, rolling out a modern AI scribe is remarkably fast. Because platforms like ScribeRunner are cloud-based and operate via existing hardware (like a smartphone), most clinics complete onboarding and physician training in less than 48 hours.
Stop Charting at Midnight. Start Living Again.
Reclaiming your time and improving patient care is no longer a waiting game. The technology is here, it is secure, and it is reshaping the healthcare landscape. Stop sacrificing your personal life to your EHR. Equip your practice with the best AI medical scribe software and get back to doing what you do best: practicing medicine.
ScribeRunner combines the best of AI technology with human oversight to deliver the most accurate, reliable medical documentation available.
Why Physicians Choose ScribeRunner:
- Hybrid AI + Human Accuracy Advanced AI reviewed by medical professionals
- 90% complete notes before patients leave
- Works with all major EHRs Epic, Athena, Cerner, and more
- HIPAA certified with bank-level 256-bit encryption
- Go live in 48 hours No complex implementation