
We don't usually talk about this openly, but most practices are silently capped.
Not capped by demand. Capped by time.
A family medicine practice owner we work with hit this wall hard. She was seeing 8 patients per day, max. Could've seen 12. The demand was there. The appointments were there. But she was charting until 8 PM most nights.
Her problem wasn't patient flow. It wasn't scheduling. It was documentation.
She was leaving money on the table because she physically couldn't chart fast enough to see more patients.
Here's what happened when she brought on a virtual scribe.
The Setup
- Practice: Solo FP + 1 PA, 1 medical assistant, 1 administrative staff
- Location: Midwest
- EHR: Athena
- Baseline: 8 patients/day, 3 days/week in clinic (24 visits/week)
- Pain point: Charting taking 2-3 hours after clinic, often until 8-9 PM
Month 1: The Adjustment
Week one was rocky. She was used to charting on her own. The idea of someone else controlling the documentation felt foreign.
But by week two, something shifted. Her scribe (assigned 1:1 with hybrid AI assistance) learned her note style. They understood her preferences. They asked clarifying questions in real-time via chat during the visit.
By end of month one: She was seeing 9 patients/day. Still adjusted, but already 12.5% more patient volume.
Month 1 impact:
- Patient volume: +12.5% (24 → 27 visits/week)
- After-hours charting: Down from 3 hours to 45 minutes
- Chart quality: Same (actually cleaner—scribe templates)
- Physician satisfaction: Medium (still getting used to it)
Month 2-3: The Breakthrough
By month two, she was comfortable delegating the charting entirely. The scribe was handling notes, prior auth requests, and follow-up coordination.
More importantly: she realized she had capacity to see more patients. The bottleneck had been her charting, not her clinical time.
She added a 4th clinic day.
Months 2-3 impact:
- Patient volume: 32 visits/week (4 days × 8 visits/day)
- After-hours work: Essentially zero (scribe finishes notes by end of clinic day)
- Prior auth requests: Being handled by scribe during clinic, not by practice staff afterward
- Physician satisfaction: High (evening time back, notes are good quality)
Month 4-6: Optimization & Growth
By month four, she'd hit a new rhythm. She was seeing 12 patients/day, 4 days/week consistently.
But the real win came when she realized something: she was doing more complex cases now because she wasn't rushed.
Why? Because she wasn't mentally fatigued from charting anxiety. Each patient got her full attention during the visit. She could slow down, ask better questions, order better diagnostics.
Her patient satisfaction scores went up. Her documentation quality improved. Her revenue grew.
She also found that having a scribe coordinating prior auth requests and insurance verifications was reducing the number of delayed approvals. Some prior auth issues that used to take 2-3 days to resolve were being flagged and submitted same-day.
Months 4-6 impact:
- Patient volume: 12 visits/day, 4 days/week = 48 visits/week (consistent)
- Revenue per week: +50% (from 24 to 36 billable visits)
- After-hours charting: Zero (scribe completes notes by 5 PM)
- Patient satisfaction: Up 8 percentage points
- Insurance approval time: Reduced from 3 days to 1 day average
- Unplanned visit cancellations: Down 12% (better scheduling coordination by scribe)
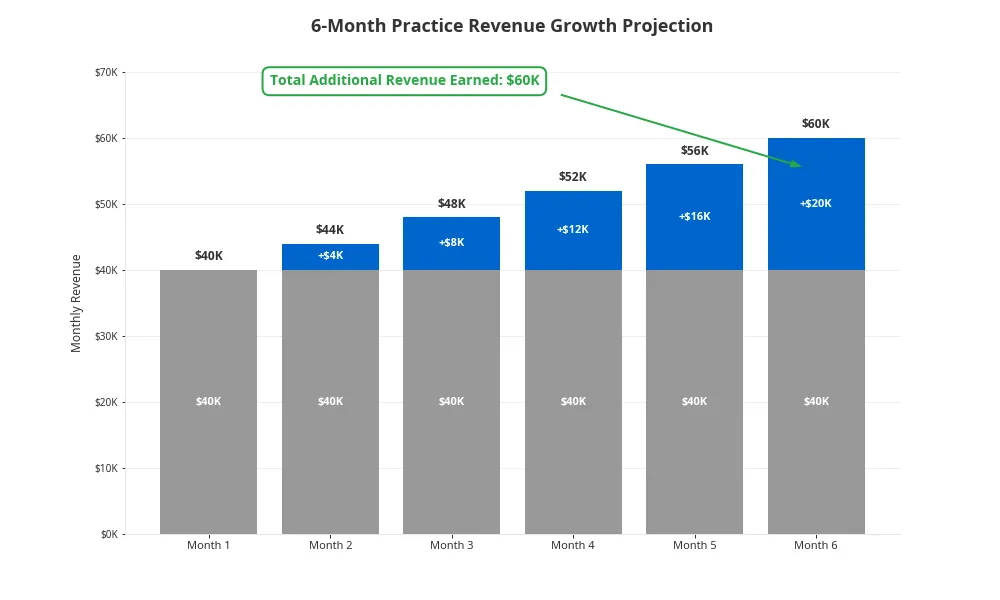
The Numbers
Let's talk about what this actually means financially.
Baseline:
- 24 visits/week × $150 avg reimbursement = $3,600/week
- Charting time: 10 hours/week (unpaid, off-hours)
After ScribeRunner:
- 48 visits/week × $150 avg reimbursement = $7,200/week
- Additional revenue: $3,600/week
- Charting time: 0 hours/week (done by scribe during clinic)
- Scribe cost: ~$2,200/month (~$550/week)
Net impact:
- Additional revenue: $3,600/week ($187,200/year)
- Scribe cost: -$550/week (-$28,600/year)
- Net annual increase: $158,600
- Plus: 10 hours/week of her personal time back
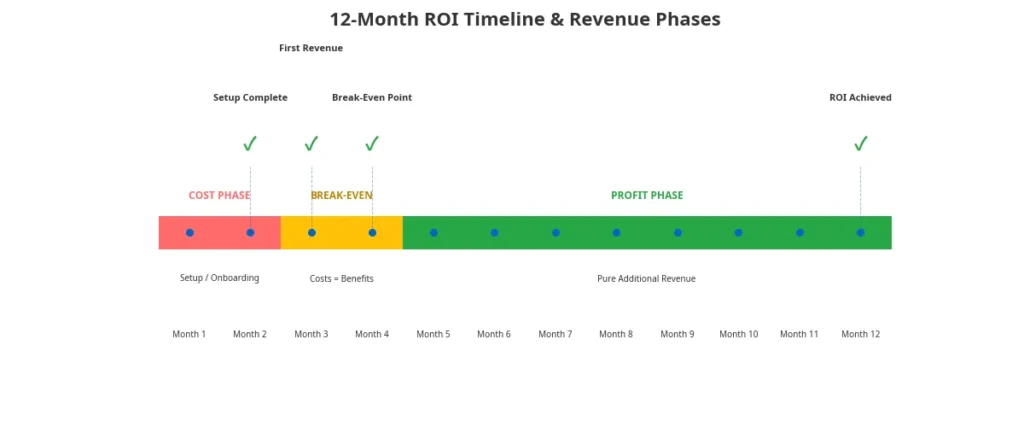
ROI:
- For every $1 spent on the scribe, she generates $6.50 in additional revenue
- Break-even point: Week 3 (scribe pays for itself in additional billing)
- Payback period: Less than a month
The Hidden Benefits
The numbers above are real. But they're not the full story.
1. Reduced Burnout
She went from charting until 8-9 PM to finishing work by 5:30 PM. That's 10 hours/week of personal time reclaimed. Over a year, that's 520 hours (13 full weeks).
For a physician, that's life-changing.
2. Better Decision-Making
When you're not exhausted from charting, you make better clinical decisions. You order the right tests. You follow up properly. You catch things you might've missed when you were rushing.
3. Continuity
Her scribe became familiar with her patient population. They started flagging patterns: "Hey, you see a lot of patients with uncontrolled hypertension. Might be a good time for a hypertension management protocol?" That's the kind of insight you only get when someone's tracking your patterns.
4. Staff Retention
Her medical assistant was spending 2-3 hours/day on prior auth, insurance verification, and scheduling chaos. Now? That's being coordinated by the scribe. The MA is actually doing patient care work (vital signs, rooming, discharge instructions). The MA's job satisfaction went up. Turnover risk went down.
5. Practice Scalability
She'd been thinking about hiring a PA to see more patients. Now she realized she didn't need to—she was already seeing more patients with the scribe. That decision saved her $120K+ in salary and benefits for a new hire.
What About the Scribe's Impact on Patients?
Here's something unexpected: patients loved it.
Her scribe (virtual, watching via screen share) was also checking patient insurance during the visit. So when a patient asked, "Will this be covered?" the scribe had the answer ready before the visit ended.
Fewer surprise bills. Fewer insurance confusion moments.
Patient satisfaction scores actually increased. Patients felt heard (the scribe took detailed notes) and they felt seen (the doctor wasn't furiously typing).
The Catch
This isn't a fairy tale. There were real adjustments:
- Weeks 1-2 were slow: Scribe was learning her style. She had to teach them her preferences. That investment up front paid off, but it required patience.
- Quality control: She had to spot-check notes the first month to ensure they matched her standards. Now it's random spot-checks only.
- Workflow change: She had to stop charting mid-visit and trust the scribe. Not everyone is comfortable with that psychological shift.
- Prior auth requests: She had to give the scribe authority to submit prior auth on her behalf (with clear guidelines). This required legal/compliance documentation.
If she'd been rigid about how things "should" be done, this wouldn't have worked. But she was willing to change.
Is This Typical?
Not everyone sees 50% revenue growth. We picked this case because it's a success story. But the pattern is consistent:
- Low-volume practices (8-12 visits/day): Usually see 25-40% volume increase
- High-volume practices (16+ visits/day): Usually see 10-15% increase (closer to max capacity already)
- Specialists: See 20-30% increase (complex cases freed up more physician time)
The gain is real. The variability depends on your starting point and how undersaturated you are with documentation burden.
The Bigger Picture
This doctor was about to hire a PA to scale her practice. Instead, she hired a virtual scribe and increased capacity 50% without adding a physician.
A PA costs $120-150K/year + benefits. A scribe costs $28-40K/year.
For a solo/small practice, that's a massive difference.
And here's the thing: the scribe scaled her productivity. The PA would have brought their own charting burden.
What Would Happen If She Stopped Using the Scribe?
She asked that question after month four.
The answer was clear: she'd drop back to 8 visits/day within a week. The charting burden would return immediately. Her evenings would be back to 8 PM finishes.
The scribe wasn't a "nice to have." It was structural to her capacity.
That's how you know it's working.
The Real Lesson
The practices that see the biggest gains from virtual scribes aren't the ones optimizing their efficiency. They're the ones realizing they've been leaving money on the table.
If you're capped by documentation time, not by demand, you're probably leaving 25-50% of potential revenue on the floor.
A virtual scribe doesn't make you more efficient. It removes the bottleneck that's preventing you from seeing the patients you already have scheduled.
That's the difference between optimization and scaling.
Is Your Practice Capped?
Ask yourself:
- Are you staying late to chart?
- Do you feel rushed during patient visits?
- Do you have open appointments that you're not filling?
- Are your staff doing insurance/prior auth work that could be automated?
- Would you see more patients if charting wasn't a bottleneck?
If you answered yes to 3+ of these, you're probably capped.
The question isn't whether a scribe would help. It's whether you're ready to uncap yourself.
Frequently Asked Questions
A: Month 1 is adjustment (5-10% increase). Months 2-3 you hit new capacity (25-40% increase). By month 4+, you're optimized. Total timeline to full growth: 3-4 months. This practice's growth was faster than average because they were significantly undersaturated.
A: Yes. A trained scribe can check insurance coverage and patient eligibility during your appointment. Many scribe systems integrate with insurance verification tools. This literally saves hours of back-office work per week.
A: Yes, but differently. You probably won't see volume growth (you're near capacity). But you'll see: zero after-hours charting, better documentation quality, reduced staff burden, and the ability to say yes to add-on visits. Plus recovery of 10-15 hours/week of personal time.
A: Absolutely. Some practices bring on a scribe but use the freed-up charting time for administration, surgery time, or just work-life balance instead of patient volume. The choice is yours.
A: In this case, scribe cost was $550/week for $3,600/week in additional revenue. That's about 15% cost of revenue on the incremental growth. Very efficient.
A: Track it for a week: How late are you staying? How many hours are you charting post-visit? If it's 2+ hours daily, charting is definitely your bottleneck. That's money on the table.
A: Most practices find patients appreciate it. Patients prefer the doctor focusing on them instead of typing insurance codes. Many patients specifically mention this in satisfaction surveys as a positive ("My doctor actually listened").
A: You could, but the numbers don't work as well. In-house scribe: $40K salary + benefits + turnover + training time. Virtual scribe: $28-40K/year flat. Plus you get backup if someone's sick. Virtual is more economical for most practices.
A: 2 weeks of setup + training. By week 3 she was fully operational. The scribe had learned her style and preferences within 2-3 weeks. This is typical.
A: Works for both. Specialists often see even bigger impact because complex cases have longer documentation times. An orthopedic surgeon charting a complex case for 20 minutes per visit? Huge opportunity.
Contact us to discuss your specialty-specific needs: